
The Link Between Family History and Your Well-Being
- November 15, 2024
Table of Contents
Maintaining good health involves more than just regular check-ups; it also requires a clear understanding of your family’s medical background. Knowing the health issues that have affected your parents, siblings, grandparents, and other relatives can provide valuable insights into potential risks you may face.
This information not only helps in identifying genetic predispositions to conditions like heart disease, diabetes, and certain cancers but also sheds light on lifestyle factors that might contribute to these illnesses.
By being aware of your history, you and your healthcare providers can take proactive steps to monitor and address health concerns before they become serious.
What is Family History?
Family history refers to the record of health information about a person and their close relatives, including parents, siblings, grandparents, and sometimes even more distant relatives. It is a way of understanding the health issues that have affected different generations within a family. This information is crucial because certain health conditions, such as heart disease, diabetes, and some cancers, can run in families due to genetic factors.
Understanding history helps doctors and patients identify potential health risks and take preventive actions. Approximately 5-10% of all diseases are hereditary, highlighting the importance of family history in identifying genetic risks.
Try it - Love it - Buy it
Avail Our Free Trial Now!
Family History: The Foundation of Medical Insights
Family history is one of the most important pieces of information for understanding a person’s health risks. By gathering detailed health information from both sides of the family, doctors can gain insight into possible health problems before they occur. This information can play a role in the prevention, early detection, and even treatment of certain diseases.
Individuals with a first-degree relative who has heart disease have a 50% higher risk of developing the condition themselves. For example, if several members of a family have experienced early-onset diabetes, this suggests that the condition may be hereditary. This knowledge can prompt early screening for the condition in the younger generations.
Medical Data:
Medical data refers to the various pieces of health information collected during patient visits, tests, and treatments. It includes quantitative data like test results and qualitative information like symptoms reported by the patient. In 2022, about 3 in 5 individuals were offered and accessed their online medical records or patient portals.
Types of Medical Data:
- Test Results: Blood tests, X-rays, MRIs, and other diagnostic results.
- Vital Signs: Measurements such as blood pressure, temperature, heart rate, and respiratory rate.
- Medications: A list of drugs a patient is currently taking or has taken in the past.
- Health Trends: Patterns over time, such as weight changes or blood sugar levels.
- Clinical Notes: Observations made by healthcare providers during consultations.
| Type of Record | Description |
|---|---|
| Electronic Health Records (EHR) | Digital records that provide a view of a patient’s health history |
| Medical History Reports | Documents that include records of past illnesses, surgeries, treatments, and family medical history |
| Treatment Records | Accounts of all treatments, therapies, and medications a patient has undergone or is receiving |
| Test Results and Imaging | Results from diagnostic tests such as blood work, MRIs, CT scans, and X-ray. |
| Surgical Reports | Documentation of any surgical procedures performed |
Medical Reports:
A medical report provides a detailed account of a patient’s health, including diagnoses, treatments, and progress. These reports are crucial for tracking the course of a patient’s condition and informing future treatment decisions. Nearly 71% of healthcare executives believe that robotics will drive the next wave of real-world services.
Key Components of a Medical Report:
- Patient Identification: Basic information like name, age, and contact details.
- Medical History: A summary of past illnesses, surgeries, and relevant family health history.
- Diagnosis: A clear statement of the patient’s condition based on tests and examinations.
- Treatment Plan: Recommendations for managing or treating the condition, including medications or lifestyle changes.
- Follow-up Instructions: Guidance on future visits or check-ups, if necessary.
Patient Records:
The patient record is an official document that stores all relevant health information about a patient. These records help healthcare providers understand a patient’s medical background and make informed decisions. As of 2021, 88.2% of office-based physicians were using any EMR/EHR system, with 77.8% having a certified EMR/EHR system..
Why Patient Records are Important:
- Continuity of Care: Helps doctors and other healthcare providers maintain a consistent view of a patient’s health.
- Monitor Health Over Time: Tracks progress, changes, and reactions to treatments.
- Prevent Medical Errors: Ensures that no important details are missed, reducing risks of incorrect treatments or duplicate tests.
- Legal and Insurance Purposes: Documents necessary for medical claims and compliance.
Medical Records: An Overview of Patient Health Information
Medical records provide a complete picture of a patient’s health over time. These records are essential for doctors to track the progression of any conditions and make informed treatment decisions.
For example, if a patient has been treated for a heart condition, the doctor can refer to previous records to understand the patient’s response to certain treatments or medications and decide the best course of action moving forward. In 2022, nearly half of individuals who accessed their online medical records (48%) did so using a website only, whereas 19% used an app only, and about one-third (32%) used both an app and a website.
An individual’s records contain all the essential data a doctor or healthcare provider needs to understand the full scope of a patient’s health. These records might include a family history, details about past surgeries, medications, allergies, and any significant health events like hospitalizations or long-term conditions such as high blood pressure or diabetes.
Key Elements:
- Patient’s details: Name, age, gender, and contact information.
- Medical history: Past illnesses, surgeries, allergies, and any ongoing treatments.
Why Medical Records Matter:
Having a complete set of medical record ensures that all health providers have the same information and can avoid mistakes like prescribing medications that interact negatively.
These records can also be used to monitor preventive care, such as vaccination schedules and routine check-ups. This helps ensure that patients are receiving the right care at the right times, avoiding unnecessary treatments, and catching potential issues before they become more serious.
Types of Medical Records and Their Importance:
There are various types of medical record, each serving a different purpose. For instance, an EHR might include test results from blood work, a record of a patient’s prescribed medications, and a doctor’s notes on treatment plans, all in one place.
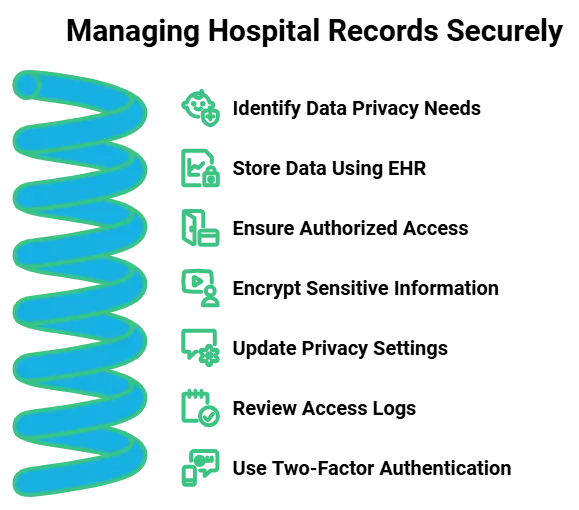
Ensuring the security and privacy of these records is crucial, as sensitive patient information must be protected from unauthorized access while remaining easily accessible to authorized healthcare providers. Some of the most common types include:
- Electronic Health Records (EHR): These are digital versions of a patient’s health records that can be easily shared between healthcare providers.
- Medical History Reports: These include detailed records of past illnesses, surgeries, and treatments.
- Test Results and Imaging: These records show the results of lab tests, X-rays, MRIs, and other diagnostic tools.
- Treatment Records: These include prescriptions, therapies, and surgeries the patient has undergone.
Each type of medical record helps doctors better understand a patient’s needs. EHRs, in particular, are important because they allow healthcare providers to quickly access and update a patient’s health information, improving the efficiency and safety of healthcare delivery.
Nearly 60% of patients are unaware of the importance of maintaining an updated family health history.
How Personal Medical Records Benefit Both Patients and Healthcare Providers:
Medical records offer numerous benefits to both patients and healthcare providers. For patients, keeping records ensures that all their health information is organized and easily accessible for future visits to different healthcare providers. This can save time, reduce errors, and provide a clearer picture of their medical history.
For healthcare providers, having access to accurate and up-to-date records allows for more informed decisions, reducing the chances of errors such as duplicate tests, incompatible treatments, or missed diagnoses. The more complete the records are, the better healthcare providers can respond to patient needs and provide appropriate care.
The genetic testing market is projected to reach $21.1 billion by 2025, driven by increasing emphasis on family health history.
How Medical Record Benefit Patients:
- Better continuity of care by having all relevant health information in one place.
- Quicker access to past treatments, making follow-ups more efficient.
How Medical Record Benefit Healthcare Providers:
- By reviewing a patient’s history, doctors can avoid prescribing medications that could cause harmful reactions or duplicate tests.
- Accurate and complete records can help protect healthcare providers from liability in case of legal disputes.
| Stakeholder | Benefits of Medical Records |
|---|---|
| Patients |
|
| Healthcare Providers |
|
History Taking: The First Step in Medical Care
What is History Taking in Healthcare?
It is one of the most important parts of the healthcare process. It involves gathering detailed information from the patient about their health, symptoms, past illnesses, and lifestyle. 90% of healthcare providers believe that access to family history through EHRs improves patient care.
This information helps doctors understand the patient’s health condition and decide what tests, treatments, or actions are needed. Family history accounts for about 10-15% of all cancer cases, emphasizing the role of genetics in cancer risk.
Talking about the history of the patient is often the first interaction between a patient and a healthcare provider, and it plays a key role in diagnosing a condition. For example, if a patient comes in with chest pain, a doctor may ask about their medical history, including whether they have ever had heart problems or if heart disease runs in their family.
With the integration of AI medical chatbots, this process can be further enhanced, as these tools can efficiently gather and analyze patient history before the consultation, aiding in the diagnostic process.
- Provides essential information for proper diagnosis.
- Helps doctors assess the overall health and potential risks of a patient.
- Forms the basis for treatment decisions, like medication or tests.
Best Practices for Effective History Taking:
To ensure that history taking is thorough, healthcare professionals must ask clear and focused questions. For example, asking the patient to describe symptoms, when they started, and any factors that make them better or worse is important for understanding the issue.
Asking about history and background of family, any ongoing medications, and previous surgeries can also provide valuable context. It is important to create a comfortable environment for the patient, as some may feel nervous about sharing sensitive health details.
50% of patients do not have a complete medical history documented, in their medical records. A good healthcare provider listens carefully, avoids interruptions, and notes down key information that can guide the diagnosis.
- Ask open-ended questions to allow patients to express themselves fully.
- Create a respectful and empathetic environment to encourage open communication.
- Take note of specific details such as symptom onset, duration, and triggers.
Hospital Records: The Core of In-Hospital Patient Care
Understanding Hospital Records and Their Use:
Hospital records are an essential part of patient care during a hospital stay. These records contain comprehensive information about the patient’s health, treatments, medications, and progress throughout their time in the hospital. Hospital record helps doctors and nurses track a patient’s recovery and make decisions about their ongoing care.
Only 30% of healthcare providers feel adequately trained to collect comprehensive family health histories. For example, if a patient is admitted for surgery, their hospital record will include details about their pre-surgery assessment, the procedure itself, and any complications or medications they need during recovery. The records help the medical team stay coordinated and focused on the patient’s needs.
- Records track a patient’s condition and progress during their hospital stay.
- Help ensure accurate communication between healthcare professionals.
- Provide a clear timeline of treatments, medications, and observations.
Components of a Hospital Records:
Hospital record usually include several key sections: personal information, medical history, admission details, diagnosis, treatment plans, and medications prescribed, test results, and notes from healthcare providers.
The personal information includes basic details such as the patient’s name, age, and contact information. Even with EHR systems in place, 43% of rural hospitals continue to rely on fax and traditional mail to send and receive patient record.
Treatment plans are the specific actions recommended by the healthcare team, while test results are documented to show progress or concerns. These records may also include the patient’s progress notes, which are updated regularly to reflect any changes in the patient’s condition.
- Includes personal and medical details to build a comprehensive profile of the patient.
- Contains treatment plans and medications prescribed for the patient’s care.
- Records progress notes and test results for ongoing monitoring.
Accurate Medical Notes and Medical Documents:
Accurate medical notes are fundamental to delivering effective patient care. These notes capture essential details about a patient’s health status, treatments administered, and responses to those treatments.
For example, a doctor might record a patient’s symptoms, diagnosis, and prescribed medications during each visit. This information ensures continuity of care, especially when multiple healthcare providers are involved. 69% of healthcare organizations are testing and implementing AI.
Organizing medical documents efficiently is equally important. Proper organization allows healthcare professionals to quickly locate and reference necessary information, which can be critical in urgent situations. Documents can be organized by patient name, visit date, or type of service provided.
For instance, keeping laboratory results, imaging reports and physician notes in a dedicated section for each patient helps streamline access and review processes. Additionally, AI-driven medical history tools can enhance document organization by automatically categorizing and indexing patient data, further improving the speed and accuracy of information retrieval.
For instance, accurate documentation of a patient’s allergy history can prevent the administration of harmful medications. Additionally, maintaining detailed and correct records supports legal compliance and protects both patients and healthcare providers in case of disputes or audits.
- Regular Audits: Conduct routine checks to verify the accuracy of records.
- Clear Handwriting or Digital Entry: Ensure that notes are legible, whether handwritten or entered electronically.
- Consistent Terminology: Use standardized medical terms to avoid confusion.
- Timely Documentation: Record information promptly to maintain up-to-date records.
- Backup Systems: Implement reliable backup methods to prevent data loss.
- Access Controls: Restrict access to sensitive documents to authorized personnel only.
Patient History:
Patient history refers to the record of a patient’s health background, which includes details about past illnesses, surgeries, hospitalizations, and ongoing treatments. This information helps healthcare providers understand a patient’s health status and any potential risks they may face based on their previous medical conditions. It also includes lifestyle factors such as diet, exercise, smoking, and alcohol use.
By reviewing a patient’s history, healthcare providers can make more informed decisions about treatment options, preventive care, and identify any patterns that may require further attention or testing.
Key Elements in Patient History:
- Medical History: Past illnesses, surgeries, hospitalizations, and treatments.
- Family History: Health conditions that run in the patient’s family, such as heart disease, diabetes, or cancer.
- Lifestyle Factors: Information about the patient’s habits, such as diet, exercise, smoking, and alcohol use.
- Allergies and Reactions: Known sensitivities to medications or environmental factors.
Case History:
Case history refers to a detailed report on a patient’s medical background, focusing on a specific condition or episode of illness. It includes all the details leading to the diagnosis and treatment of that condition.
Components:
- Presenting Complaint: The symptoms or concerns the patient has when visiting the healthcare provider.
- Medical Investigation: Tests, procedures, and consultations that help diagnose the condition.
- Treatment and Outcome: The medications, surgeries, or therapies used, along with how the patient responded to them.
- Prognosis: The expected course of the condition, including possible complications or recovery timelines.
Past Medical History and Medicine History Documentation:
Recording a patient’s past medical history is essential for understanding their overall health and identifying potential risk factors. This history includes previous illnesses, surgeries, hospitalizations, and chronic conditions.
For example, knowing that a patient has a history of diabetes can influence current treatment decisions and monitoring strategies. Accurate past records help healthcare providers anticipate possible complications and tailor care plans accordingly.
Tracking medicine history involves documenting all medications a patient has taken, including prescriptions, over-the-counter drugs, and supplements. This information is crucial for avoiding drug interactions and ensuring that medications are used safely and effectively.
For instance, if a patient is taking blood thinners, a doctor needs to be aware to adjust dosages when prescribing new medications. In 2020, 41% of individuals accessed their online records or patient portals, indicating a growing trend in patient engagement with digital health tools.
Analyzing past medical events allows healthcare professionals to recognize trends and make informed decisions about a patient’s current and future care. By reviewing previous health issues and treatments, providers can assess the effectiveness of past interventions and adjust strategies as needed.
Elements of Past Medical History:
| Key Elements | Description |
|---|---|
| Previous Illnesses | Past illnesses and treatments. |
| Hospitalizations | Record of surgeries or hospital stays. |
| Chronic Conditions | Long-term conditions like diabetes, hypertension. |
| Medication History | Medications used, OTC drugs, and supplements. |
| Family Medical History | Health conditions that run in the family, like genetic or hereditary diseases. |
About 70% of patients express concerns regarding the privacy and security of their electronic records. For example, if a patient has repeatedly experienced adverse reactions to a specific medication, alternative treatments can be considered. Integrating past history into current care ensures a comprehensive approach to patient health.
- Questionnaires: Use detailed forms to gather complete medical and medication histories.
- Patient Interviews: Conduct thorough interviews to capture nuances not covered in written records.
- Electronic Health Records (EHR): Utilize EHR systems to maintain and update histories efficiently.
- Family Medical History: Include information about relatives’ health to identify hereditary conditions.
- Lifestyle Factors: Document factors like smoking, alcohol use, and exercise habits that affect health.
- Allergy Documentation: Clearly note any known allergies to medications or substances.
Personal Health Records Management:
Maintaining personal records is important for both patients and healthcare providers. These records include information such as medical history, test results, vaccination records, and treatment plans.
By keeping comprehensive personal health records, patients can easily share their health information with different healthcare professionals, ensuring coordinated and informed care. Patients who actively manage and share their family health history are 20% more likely to engage in preventive health behaviors.
Patients should be able to view their records through online portals or request copies from their healthcare providers. Easy access empowers patients to take an active role in their healthcare decisions.
For instance, having access to lab results allows patients to discuss findings with their doctors promptly and understand their health status better.
Updating personal health information regularly ensures that records remain current and accurate. Patients should review their records periodically to add new information, correct any errors, and remove outdated data. This ongoing maintenance helps prevent miscommunications and ensures that all healthcare providers have the latest information.
- Secure Online Portals: Provide encrypted platforms for patients to access their records safely.
- Mobile Access: Enable access to health records via smartphones and tablets for convenience.
- Educational Resources: Include informational materials to help patients understand their health data.
- Notification Systems: Alert patients when their records are updated or accessed.
- Data Portability: Allow patients to easily transfer their records between different healthcare providers.
Medical History Forms and Patient Medical History Forms:
Designing effective medical history forms is key to collecting accurate patient information. These forms should be user-friendly and structured to capture all relevant health details, including past illnesses, surgeries, medications, and family medical history.
For example, a well-designed form might include sections for chronic conditions, recent hospitalizations, and current medications to ensure nothing is overlooked during the patient intake process.
Implementing patient medical history forms involves integrating them into the healthcare workflow, whether through paper-based methods or electronic systems. Efficient implementation ensures that forms are completed accurately and submitted promptly.
The use of Enterprise AI Solutions can further enhance this process by automating data entry, verifying information, and ensuring that patient histories are accurately captured and integrated into the system, improving efficiency and reducing errors.
For instance, using digital forms that patients can fill out online before their appointment can save time and reduce errors. Training staff on how to handle and process these forms is also essential for smooth operations.
- Mandatory Fields: Include essential questions that must be answered to ensure completeness.
- Skip Logic: Use conditional questions to streamline the form based on previous answers.
- Multilingual Options: Provide forms in multiple languages to accommodate diverse patient populations.
- Accessible Formats: Ensure forms are available in formats accessible to individuals with disabilities.
- Clear Instructions: Offer guidance on how to complete each section of the form accurately.
- Review Sections: Include areas for patients to add additional comments or clarify responses.
Mental Health Records and Medical Timeline Tracking:
Maintaining mental health records is crucial for providing comprehensive care to patients with mental health needs. These records include information about diagnoses, treatment plans, therapy sessions, and progress notes.
For example, a therapist might document a patient’s progress in managing anxiety through cognitive-behavioral therapy sessions. Detailed records help ensure that patients receive consistent and effective treatment over time.
Integrating a medical timeline into records allows healthcare providers to visualize a patient’s health journey, including significant events and changes in their condition. A medical timeline can highlight periods of improvement or relapse, helping providers identify patterns and triggers.
For instance, tracking a patient’s mood over several months can reveal correlations between life events and mental health fluctuations.
In a study, it was discovered that 76% of patients could be accurately diagnosed based solely on their medical history, 12% required a physical examination for diagnosis, and 11% needed laboratory tests.
Tracking mental health progress involves regularly updating records with new information about a patient’s status and responses to treatment. This ongoing monitoring helps assess the effectiveness of interventions and make necessary adjustments.
- Confidentiality Measures: Implement strict protocols to protect the privacy of mental health records.
- Collaborative Notes: Allow multiple providers to contribute to a patient’s records for a holistic view.
- Outcome Tracking: Record specific metrics to evaluate the success of mental health interventions.
- Crisis Documentation: Include detailed notes on any mental health crises and the responses provided.
- Therapeutic Goals: Clearly outline and update the goals set for therapy and track progress towards them.
- Patient Feedback: Incorporate patient-reported outcomes and feedback to enhance care quality.
Subscribe to our Newsletter!
Subscribe our Newsletter to stay updated
Conclusion:
Understanding your history and keeping accurate medical records are vital steps in managing your health effectively. By being aware of any hereditary conditions, you and your healthcare team can take necessary precautions to monitor and address potential health issues early on.
This proactive approach can lead to better health outcomes and a higher quality of life. People with a history of diabetes are 40% more likely to undergo regular screening for the disease.
Moreover, maintaining detailed records ensures that all relevant health information is readily available when needed. This continuity of information helps healthcare providers make informed decisions about your care, leading to more personalized and effective treatments. Documenting and Updating your history and medical records is an investment in your long-term health and well-being.
Read More Blogs
See what’s trending in the medical world with our blogs.


